Aging population around the world leads to an increasing incidence of degenerative spinal conditions. Minimally invasive spine surgery is becoming popular with its proposed benefit of lower infection rate, shorter hospital stay, less blood loss, less perioperative pain and early return to work [1] .

Minimally Invasive Surgery vs Endoscopic Surgery
Minimally invasive spine surgery is a loose term which means surgery perform with a smaller scar with target soft tissue damage. It ranges from using a specialized retractor or using a tube to retract muscles with the help of microscope. Traditional large size open instruments can be used to perform surgery.
The aim is less soft tissue damage, however, in order to see the target area in spine, soft tissue needs to be burnt and removed between the skin and the target site to allow microscope to see the target area. Some of the examples of minimally invasive spine surgeries are oblique lateral lumbar interbody fusion, extreme lateral lumbar interbody fusion, minimally invasive (MIS) tubular decompression or fusion, MIS mini-open decompression and/or fusion.
All of these surgeries generally are still consider open surgery as the patient required to make an open wound sufficient to be visualized by microscope (Figure 1). All the soft tissue (skin retracted, muscles removed/retracted), bone/facet joint removed with or without nerve retracted by assistant surgeon before we can visualize the area of target under microscope, naked surgeon’s eyes with or without loupes. Most if not all minimally invasive spinal surgery required general anesthesia.
What is endoscopic spine surgery
Endoscopic spine surgery is one of the least invasive version of minimally invasive spine surgery. Some surgeons term it as the bridge between pain procedure and traditional open spinal surgery.
It involves the use of an endoscope which is a 8-10mm in diameter with 4 functions:
- Irrigation – the inflow of saline from inflow port constantly washout tissue and blood clots that is required to be removed.
- Magnification by lens – to improve safety and to visualize nervous tissue clearly.
- Light source – to provide clear visualization.
- Working channel – delicate endoscopic instruments can be passed into a small working channel in an endoscope to reach the target disc, bone, nerve region to perform surgery.
As spinal endoscope can be inserted in minimally traumatic fashion directly on target bony region, bypassing soft tissue to prevent repetitive trauma to soft tissue, endoscopic spine surgeon can “dock” on the area of target to minimize collateral damage. As the lens is in the front of endoscope directly hovering the target area rather than 50cm away from skin, there is minimal dissection or burning of tissue between skin and target area. As endoscope is small in size, it can fit into natural spinal cavity such as spinal foramen to perform decompression of nerves and remove herniated disc.
Due to the abovementioned reasons, it can be performed under local anesthesia with moderate sedation.
One port endoscope (Figure 1) or two ports endoscopic procedures (Figure 2) can also be used to fit in the natural window use of midline lower back used in traditional spine surgery with one or two subcentimeter incisions to perform more complex procedure such as revision spinal canal decompression, interbody fusion procedure, washing out of infective tissue in spine, tumor procedures.
Dr. Wu Pang Hung has established a protocol to perform day surgeries for patients who presented with sciatica (herniated disc /prolapsed intervertebral disc), spinal stenosis, and cervical radiculopathy and in selected cervical and thoracic myelopathy patients with endoscopic spine surgery in Singapore and advised given to overseas centres to set up their practice. Here are some of the references of articles he wrote which described these procedures [2-6].
Visual examples
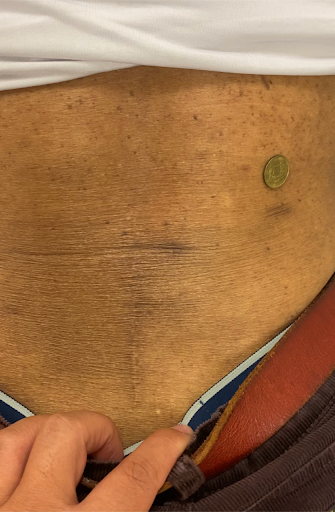
Figure 1
The horizontal incision is the wound required for one port (uniportal) transforaminal endoscopic revision lumbar four lumbar five discectomy in a patient who had previous open lumbar four lumbar five microdiscectomy (midline scar).
In our experience, we find that endoscopic surgery through the transforaminal route is a good treatment strategy for patient who had recurrence disc when we can avoid the scar and lower the risk of spinal injury and dura leak compared to conventional revision open posterior surgery.

Figure 2
Postoperative day 14 scar of 2 ports unilateral biportal endoscopic decompression of lumbar two lumbar three in a patient who had previous lumbar three lumbar four open decompression.
We can perform revision spinal decompression surgery for patients who had previous open spine surgery with a smaller wound and less traumatic experience as a day surgery.
Types of Procedure
Endoscopic spine surgery is divided into uniportal and biportal endoscopic spine surgery[8]. Due to evolution of endoscopic spine surgical technique, more and more conditions can be treated endoscopically as a day procedure.
In Achieve Spine and Orthopaedic Centre, we can convert up to 80% of our load of traditional open spinal surgery to endoscopic spine surgery. In selected cases, they can be performed as outpatient day surgery centre procedures. As learning curve of spinal endoscopy is steep, patient needs to speak to spinal surgeon to decide whether he/she is suitable for endoscopic spine surgery in their practice.
Here is the table according to the region of the body and the common description of the endoscopic spine surgery. Those 🟢 can be performed under local anesthesia:
Lumbar
| Anatomy (indications) | Uniportal | Biportal |
|---|---|---|
|
Extraforamen (Prolapsed disc, Bertolotti syndrome, adjustment of interbody cages) |
🟢 Extraforaminal endoscopic lumbar discectomy (EELD) |
Far lateral approach/ paraspinal approach unilateral biportal endoscopy
(Video 1) Adopted with thanks
from International Society Of
Unilateral Biportal Endoscopy
Henan 2021 |
|
Foramen (Prolapsed disc, foraminal stenosis, adjustment of interbody cages) |
🟢 Transforaminal endoscopic lumbar discectomy (TELD)
Adopted with thanks from 6th Asean
MISST meeting in 2021 |
Far lateral approach/ paraspinal approach unilateral biportal endoscopy |
|
Lateral Recess (spinal stenosis,adjacent segment degeneration, prolapsed disc, facet cyst, discal cyst) |
🟢 Transforaminal endoscopic lateral recess decompression (TELRD)
Lumbar endoscopic lateral recess decompression (LELRD) |
Unilateral Biportal Endoscopic interlaminar approach (UBE) |
|
Central Canal with or without contralateral lateral recess (spinal stenosis, adjacent segment degeneration, prolapsed disc, facet cyst, discal cyst) |
Interlaminar Contralateral Endoscopic Lumbar Foraminotomy (ICELF) [9] adopted with thanks from Wu, P. H.; Kim, H. S.; Jang, I.-T., How I do it? Uniportal full endoscopic contralateral approach for lumbar foraminal stenosis with double crush syndrome. Acta Neurochirurgica 2020, 162, (2), 305-310. |
Unilateral Biportal Endoscopic interlaminar approach (UBE) |
|
Interbody Fusion |
Uniportal Posterolateral endoscopic interbody fusion[10] Adopted with thanks from Uniportal Endoscopic Lateral to Medial Direction Transforaminal Lumbar Interbody Fusion: A Case Report and Technical Guide for Navigating Through Landmarks in Left Lumbar 4/5 Post Laminotomy Revision Lumbar Fusion Surgery. J Minim Invasive Spine Surg Tech 2021, 6, (1), 66- 73. |
Biportal posterolateral endoscopic lumbar interbody fusion. Adopted with thanks from International Society of Unilateral Biportal Endoscopy Talk in Xinjiang China in March 2022. |
|
Others (for advanced level surgery) |
Tumor resection, infection and debridement |
Tumor resection, infection and debridement UBE assisted fusion and/or osteotomy in deformity correction |
Price

As endoscopic spine surgery can be performed as day surgery and shorten hospital stays with a very low infection rate and simple protocol of perioperative management. Large randomized cohort studies and retrospective studies show it is more cost-effective than open spinal surgery from societal perspective [14-16] and it is challenging traditional spine surgery as the new gold standard[17].
Endoscopic spine surgery however requires specialized and delicate endoscopic equipment and consumable to perform surgery which is unlike open spinal surgery which can use large traditional equipment[18, 19].
Each type of endoscopic spine surgery required different types of approach and equipment, discuss with an experienced endoscopic spine surgeon to decide what is suitable to your needs and the cost it requires.
Recovery Time

Wu et al compared his early series of uniportal and biportal endoscopic spine surgery result during his learning curve period and found the average length of stay for 90% of his patients are within 23 hours[2]. The quick recovery allows patients to walk within hours after surgery and typically does not require urinary catherization and calf pump.
Many endoscopic spine patients can go home within 6 -8 hours of surgery[2].
Long Term Success Rate
Success of endoscopic spine surgery is comparable to open surgery in terms of long term pain relief, some of the conditions such as thoracic prolapsed disc [7, 11] which typically required open chest approach, resection of bone and perhaps screws fixation as well as lumbar foraminal pathologies[9] which required decompression and/or fusion procedure[20, 21]. These procedures can be performed with endoscopy as day surgery in selected cases.
Endoscopic spine surgery is a sub specialization of spine surgery with significant learning curve [19, 22], it is in best interest for the patient to speak to endoscopic spine surgeon to discuss the success rate of surgery.
Achieve Spine And Orthopaedic Centre is not advocating that endoscopic spine surgery is the best option for all spine cases and spinal endoscopy cannot replace all traditional open spinal surgery. Our doctors are experienced in open spinal surgery which is required for some of the more complicated cases of spinal surgery. However endoscopic spine surgery can replace 80% of conditions requiring open spine surgery in our experience
References
- Kim, H. S.; Wu, P. H.; Jang, I.-T., Current and Future of Endoscopic Spine Surgery: What are the Common Procedures we Have Now and What Lies Ahead? World Neurosurgery 2020, 140, 642-653.
- Wu, P. H.; Chin, B. Z. J., Ambulatory uniportal versus biportal endoscopic unilateral laminotomy with bilateral decompression for lumbar spinal stenosis-cohort study using a prospective registry. 2023.
- Wu, P. H.; Kim, H. S.; Lee, Y. J.; Kim, D. H.; Lee, J. H.; Yang, K.-H.; Raorane, H. D.; Jang, I.-T., Posterior endoscopic cervical foramiotomy and discectomy: clinical and radiological computer tomography evaluation on the bony effect of decompression with 2 years follow-up. European Spine Journal 2020.
- Hung, D. W. P.; Kavishwar, D. R. A.; Natalie, D. T. H. W.; Tan, D. G., Unilateral Biportal Endoscopic Supralaminar, Posterior Spinous Process Sparing Approach For En Bloc Cervical Laminectomy In Case Of Cervical Osteochondroma Causing Myelopathy A Case Report. North American Spine Society Journal (NASSJ) 2023, 100225.
- Lau, E. T.; Wu, P. H., Technical Note on Unilateral Biportal Lumbar Endoscopic Interbody Fusion. In Surgical Techniques Development, 2022; Vol. 11, pp 71-89.
- Wu, P. H.; Kim, H. S., Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. 2020, 21, (6).
- Wu, P. H.; Kim, H. S.; Kim, J.-Y.; Lee, Y. J.; Kim, D. H.; Lee, J. H.; Jeon, J. B.; Jang, I.-T., Uniportal thoracic endoscopic decompression using one block resection technique for thoracic ossified ligamentum flavum technical report. Interdisciplinary Neurosurgery 2021, 23, 100963.
- Hofstetter, C. P.; Ahn, Y.; Choi, G.; Gibson, J. N. A.; Ruetten, S.; Zhou, Y.; Li, Z. Z.; Siepe, C. J.; Wagner, R.; Lee, J.-H.; Sairyo, K.; Choi, K. C.; Chen, C.-M.; Telfeian, A. E.; Zhang, X.; Banhot, A.; Lokhande, P. V.; Prada, N.; Shen, J.; Cortinas, F. C.; Brooks, N. P.; Van Daele, P.; Kotheeranurak, V.; Hasan, S.; Keorochana, G.; Assous, M.; Härtl, R.; Kim, J.-S., AOSpine Consensus Paper on Nomenclature for Working-Channel Endoscopic Spinal Procedures. Global spine journal 2020, 10, (2 Suppl), 111S-121S.
- Wu, P. H.; Kim, H. S.; Jang, I.-T., How I do it? Uniportal full endoscopic contralateral approach for lumbar foraminal stenosis with double crush syndrome. Acta Neurochirurgica 2020, 162, (2), 305-310.
- Wu, P. H.; Kim, H. S.; Jang, I.-T., Uniportal Endoscopic Lateral to Medial Direction Transforaminal Lumbar Interbody Fusion: A Case Report and Technical Guide for Navigating Through Landmarks in Left Lumbar 4/5 Post Laminotomy Revision Lumbar Fusion Surgery. J Minim Invasive Spine Surg Tech 2021, 6, (1), 66-73.
- Wu, P. H.; Kim, H. S.; Raorane, H. D.; Heo, D. H.; Yi, Y. J.; Yang, K.-H.; Jang, I.-T., Safe Extraforaminal Docking and Floating Technique in Transforaminal Endoscopic Discectomy for Thoracolumbar Junction for Calcified Disc Herniation: A Case Report and Technical Review Junction for Calcified Disc Herniation. J Minim Invasive Spine Surg Tech 2020, 5, (1), 26-30.
- Kim, H. S.; Wu, P. H., Comparative Clinical and Radiographic Cohort Study: Uniportal Thoracic Endoscopic Laminotomy With Bilateral Decompression by Using the 1-Block Resection Technique and Thoracic Open Laminotomy With Bilateral Decompression for Thoracic Ossified Ligamentum Flavum. 2022.
- George, R.; Wu, P. H., Posterior Cervical Unilateral Biportal Endoscopic One-Block Resection Technique for Cervical Ossified Ligamentum Flavum. In Surgical Techniques Development, 2023; Vol. 12, pp 80-86.
- Gadjradj, P. S.; Broulikova, H. M.; van Dongen, J. M.; Rubinstein, S. M.; Depauw, P. R.; Vleggeert, C.; Seiger, A.; Peul, W. C.; van Susante, J. L.; van Tulder, M. W.; Harhangi, B. S., Cost-effectiveness of full endoscopic versus open discectomy for sciatica. British journal of sports medicine 2022, 56, (18), 1018-25.
- Choi, K. C.; Shim, H. K.; Kim, J. S.; Cha, K. H.; Lee, D. C.; Kim, E. R.; Kim, M. J.; Park, C. K., Cost-effectiveness of microdiscectomy versus endoscopic discectomy for lumbar disc herniation. The spine journal : official journal of the North American Spine Society 2019, 19, (7), 1162-1169.
- Wang, D.; Xie, W.; Cao, W.; He, S.; Fan, G.; Zhang, H., A Cost-utility Analysis of Percutaneous Endoscopic Lumbar Discectomy for L5-S1 Lumbar Disc Herniation: Transforaminal versus Interlaminar. Spine (Phila Pa 1976) 2019, 44, (8), 563-570.
- Gadjradj, P. S., Full-endoscopic lumbar disc surgery: the new gold standard? (PhD Academy Award). British journal of sports medicine 2022.
- Sebastian, R.; Martin, K.; Harry, M.; Georgios, G., Use of newly developed instruments and endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. Journal of Neurosurgery: Spine SPI 2007, 6, (6), 521-530.
- Wu, P. H.; Kim, H. S.; Choi, D. J.; Gamaliel, Y.-H. T., Overview of Tips in Overcoming Learning Curve in Uniportal and Biportal Endoscopic Spine Surgery. J Minim Invasive Spine Surg Tech 2021, 6, (Suppl 1), S84-S96.
- Wu, P. H.; Kim, H. S.; An, J. W.; Kim, M.; Lee, I.; Park, J. S.; Lee, J. H.; Kang, S.; Lee, J.; Yi, Y.; Lee, J. H.; Park, J. H.; Lim, J. H.; Jang, I.-T., Prospective Cohort Study with a 2-Year Follow-up of Clinical Results, Fusion rate, and Muscle Bulk for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion. Asian Spine J 2023, 0.
- Kim, H.-S.; Wu, P.-H.; An, J.-W.; Lee, Y.-J.; Lee, J.-H.; Kim, M.-H.; Lee, I.; Park, J.-S.; Lee, J.-H.; Park, J.-H.; Jang, I.-T., Evaluation of Two Methods (Inside-Out/Outside-In) Inferior Articular Process Resection for Uniportal Full Endoscopic Posterolateral Transforaminal Lumbar Interbody Fusion: Technical Note. Brain sciences 2021, 11, (9), 1169.
- Wu, P. H., Early Career Challenges in Setting Up an Endoscopic Spine Surgery Practice. World Neurosurgery 2020, 144, 264-269.


